

Toasted skin syndrome is not a condition most people have heard of until they find themselves searching for an explanation. A mottled, net-like discolouration usually appears on the thighs, shins, abdomen, or lower back, and the connection to a laptop, hot water bottle, or heating pad is not immediately obvious. It is a straightforward condition in many respects, but it is also frequently misunderstood, misattributed, or discovered only after it has been present for some time.
Medically known as erythema ab igne, the condition has been documented for well over a century. What has changed is the context in which it appears. Once associated primarily with industrial heat exposure and open fires, it is now most commonly seen in people managing chronic pain with heat therapy, those who use laptops on their laps for extended periods, and older adults who rely on space heaters or electric blankets for warmth. In the UK, where hot water bottles and electric blankets are household staples, it is more relevant than its relative obscurity might suggest.
Understanding the condition properly matters for a practical reason: early identification and a straightforward change in eating habits is usually all that is needed to prevent it from progressing. Left unrecognised, however, it can lead to permanent pigmentation and in rare, long-standing cases, more significant skin changes that warrant medical review. This guide covers the full picture, from what the rash looks like and why it develops, through to treatment options, realistic recovery expectations, and clear guidance on when to seek professional advice.
The most useful place to start is with a clear explanation of what toasted skin syndrome actually is, and why it has become more common in modern domestic settings.
Your Toasted Skin Syndrome Questions
Real Questions from Real People - Answered
Straightforward answers to the questions people like you are asking right now about Toasted Skin Syndrome.

Be the first to ask a Toasted Skin Syndrome question.
Click here to ask your own question.
Find A Verified Clinic
Trusted Toasted Skin Syndrome Experts, Local to You
Easily connect with qualified, verified professionals for safe, reliable treatment.

To find a Toasted Skin Syndrome clinic near you, please click here.
What Is Toasted Skin Syndrome?
Toasted skin syndrome (erythema ab igne) is caused by repeated heat exposure. Learn how it develops, why it is becoming more common, and what happens to the skin.

Toasted skin syndrome is a skin condition caused by repeated, prolonged exposure to low-level heat - warm enough to damage skin tissue over time, but not hot enough to cause an immediate burn. Its medical name is erythema ab igne, a Latin phrase meaning "redness from fire," and while the condition is not new, it is becoming more commonly seen in everyday settings far removed from its historical origins.
A condition with a long history and a modern relevance
Erythema ab igne was first documented in people who worked close to intense heat sources: bakers, ironworkers, and those who spent long hours beside open fires or coal stoves. Central heating and changes in working conditions made it relatively uncommon for several decades. It has since re-entered clinical attention, this time linked to the kinds of heat sources found in most UK homes and workplaces - laptops, electric blankets, heating pads, and hot water bottles.
The condition has not changed. The heat sources causing it have.
What actually happens to the skin
The damage is cumulative rather than immediate. When skin is exposed to the same localised heat source repeatedly - over weeks or months - it undergoes gradual change at a cellular level. The heat disrupts the superficial blood vessels beneath the skin's surface, damages elastic fibres, and triggers the release of melanin and haemosiderin (a pigment produced when red blood cells break down). These deposits accumulate in the skin and produce the characteristic discolouration associated with the condition.
The critical temperature range is generally cited between 43°C and 47°C. That is warm rather than hot - comparable to a heating pad set to medium, a laptop running under load, or a hot water bottle that has cooled slightly but remains in contact with skin for an extended period.
Why it often goes unnoticed at first
Because toasted skin syndrome develops gradually, many people do not connect the rash to a heat source immediately. The early stages are subtle: a faint, blotchy redness that fades when the heat is removed. It can be easy to dismiss as irritation or a minor reaction. It is only with continued exposure - and the progression to a persistent, net-like pattern of discolouration - that most people seek an explanation.
On darker skin tones, the initial redness may be particularly difficult to detect, which can delay recognition further.
Understanding what toasted skin syndrome is, and how it develops, is the first step towards identifying it early and taking straightforward action before changes become more difficult to reverse.
What Does Toasted Skin Syndrome Look Like?
Toasted skin syndrome starts as blotchy redness and develops into a net-like brown pattern. Learn how it progresses and where it typically appears.
Knowing what to look for is often the first step towards getting the right answer. The appearance of toasted skin syndrome is distinctive, but it develops in stages, and in the early phase, it can be easy to overlook or misattribute to something else.
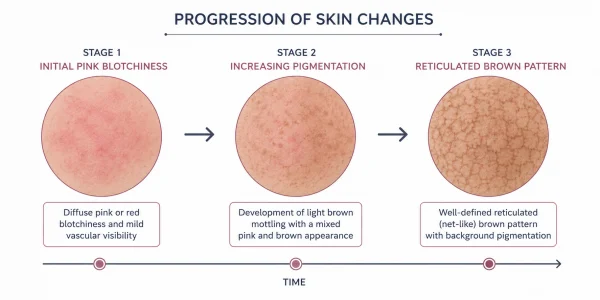
How the rash develops over time
The initial presentation is transient, blotchy redness in the area of skin in direct contact with the heat source. At this stage, the redness is blanchable-meaning it fades temporarily when pressure is applied-and typically disappears once the heat source is removed. Many people do not seek advice at this point, often assuming the redness is a minor reaction that will resolve on its own.
With continued exposure, the rash becomes persistent. The blanchable redness gives way to a fixed discolouration, and the pattern becomes more defined. This is the stage most associated with toasted skin syndrome: a reticulated, net-like or lace-like pattern that follows the underlying network of superficial blood vessels. The colour shifts from red or pink towards brown, purple-brown, or a deeper grey-brown depending on skin tone and the duration of exposure.
In more advanced or long-standing cases, the skin may also show:
- Telangiectasias (small, visibly dilated blood vessels at the surface)
- Epidermal atrophy (a slight thinning or texture change in the affected area)
- Persistent discolouration that no longer fades between heat exposures
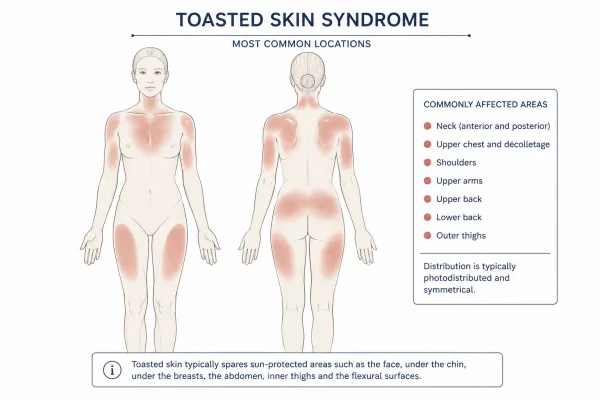
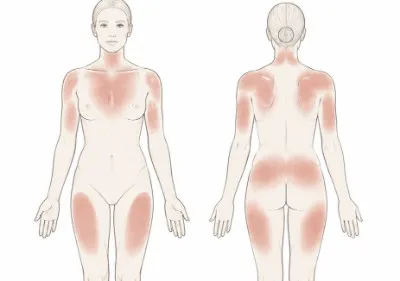
Where on the body does it appear?
The rash appears wherever the heat source has been in direct, regular contact with the skin. Common locations include:
- The front of the shins and lower legs (from space heaters, fires, or radiators)
- The inner thighs or lap area (from laptops)
- The abdomen or lower back (from heating pads or hot water bottles)
- The upper back (from heated car seats)
The location is often a useful diagnostic clue in itself.
Does it look different on darker skin tones?
This is a clinically relevant consideration that is often overlooked. On lighter skin, the initial erythema (redness) tends to be visually apparent relatively early. On darker skin tones, the early redness can be significantly harder to detect, so the condition may go unrecognised until the pigmentation advances to a more noticeable brown or grey-brown discolouration. Anyone who uses heat sources regularly and notices any change in skin texture or tone in those areas — regardless of how subtle - should be investigated further.
The net-like pattern, once established, is generally recognisable across all skin tones, though the contrast against the surrounding skin will vary.
The appearance of toasted skin syndrome is consistent enough that a clinical diagnosis can usually be made based on the rash's pattern and a straightforward history of heat exposure.
What Causes Toasted Skin Syndrome?
Toasted skin syndrome results from repeated low-level heat exposure. Learn which everyday devices are most commonly responsible and why the damage accumulates.

Toasted skin syndrome has a single, consistent cause: repeated, direct contact with a localised heat source over a sustained period. What has changed over time is not the mechanism, but the heat sources involved. Understanding which everyday items carry a risk - and why - makes it considerably easier to take preventive action.
The heat threshold that matters
The damage does not require extreme heat. Research consistently identifies the critical temperature range as 43°C to 47°C - warm rather than hot, and well below the threshold that would cause an immediate burn. At these temperatures, skin does not send the urgent pain signals associated with a scald or burn, which is part of why the exposure continues unchecked. The damage accumulates gradually, over repeated sessions, rather than resulting from a single incident.
Duration and frequency matter as much as temperature. Occasional use of a heating pad for 20 minutes is unlikely to cause problems. The same heating pad used for several hours daily, over weeks or months, is a different matter.
Modern heat sources most commonly responsible
The heat sources most frequently associated with toasted skin syndrome today include:
- Laptops: Particularly when rested directly on the thighs or abdomen for extended periods. The underside of a laptop running under load can reach temperatures well within the implicated range.
- Heating pads and electric heat pads: Widely used for back pain, period pain, and muscle relief. The risk increases with higher settings and prolonged use against bare skin.
- Hot water bottles: Common in UK households, particularly in colder months. The risk is greatest when the bottle is used at high temperatures or kept in contact with the skin for extended periods while sleeping or resting.
- Electric blankets: Used overnight or for extended periods, these can sustain skin exposure to low-level heat for far longer than other sources.
- Space heaters: Historically associated with shin presentations in older adults who sit close to a heat source for warmth. Still a relevant cause in UK homes.
- Heated car seats: An increasingly reported cause, particularly among people with long commutes who use seat warmers regularly throughout the year.
Occupational and historical context
In earlier decades, toasted skin syndrome was largely an occupational condition - seen in bakers, glassblowers, metalworkers, and others exposed to industrial heat sources as part of their working day. That context still applies in some settings, but it no longer represents the majority of cases seen clinically. Most presentations today are domestic, often linked to pain management habits or extended device use.
That shift is worth understanding because it means the condition no longer fits a clear demographic profile. It can affect anyone who regularly uses the heat sources listed above, regardless of age or occupation.
Why is the damage cumulative?
Each exposure session causes a small degree of stress to the superficial blood vessels and skin cells in the affected area. In isolation, this is not significant. Repeated consistently over time, however, the damage accumulates: vessels become permanently dilated, elastic fibres degrade, and pigment-producing cells are disrupted. The result is the reticulated discolouration characteristic of the condition.
This also explains why early intervention matters. Removing the heat source in the early stages - before structural changes to the skin have consolidated - gives the skin a reasonable opportunity to recover. Waiting until the pigmentation is well established reduces that likelihood.
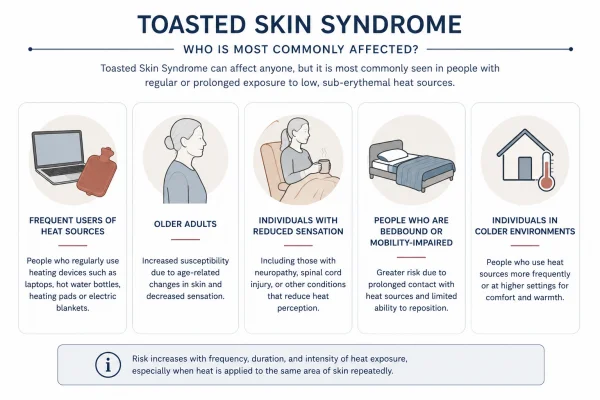
Who Is Most Likely To Develop Toasted Skin Syndrome?
Toasted skin syndrome is more common in women, older adults, and people managing chronic pain. Find out which habits and conditions increase the risk.

Toasted skin syndrome can affect anyone who uses heat sources regularly and directly against their skin. That said, certain patterns of behaviour and certain health conditions make some people meaningfully more likely to develop it than others. Recognising those risk factors is useful - not to cause concern, but to help people make more informed decisions about how they use heat day to day.
Women and people managing chronic pain
The condition is more prevalent in women than in men, a pattern consistent across historical and contemporary case data. This is partly explained by heat use habits: women are statistically more likely to use hot water bottles, heating pads, and electric blankets - particularly to manage menstrual pain, pelvic discomfort, and musculoskeletal conditions.
People managing chronic pain more broadly represent a significant proportion of those affected. The connection is straightforward: heat is a genuine and effective short-term analgesic, and those dealing with persistent pain often rely on it heavily and regularly. The same therapeutic habit that provides relief can, over time, produce cumulative skin damage in the area of application.
The chronic pain connection in more detail
This is an aspect of toasted skin syndrome that receives relatively little attention in general health content, but it is clinically well-documented and practically important.
Conditions associated with an elevated risk include:
- Endometriosis and chronic pelvic pain: A 2025 narrative review published in the journal Life (MDPI) examined erythema ab igne specifically as a potential cutaneous marker of chronic heat use in patients with endometriosis - noting that between 40% and 87% of those with chronic pelvic pain have the condition, and that heat therapy is among the most common self-management strategies used.
- Back pain and musculoskeletal conditions: Prolonged use of heating pads or heat wraps applied to the lower back is a well-recognised cause, particularly where pain has been ongoing for months or years.
- Fibromyalgia and other pain syndromes: Where heat provides broader symptomatic relief, use tends to be both frequent and sustained - a pattern that carries a higher cumulative risk.
The practical tension here is worth acknowledging. Heat therapy is not inadvisable. It is a reasonable and widely recommended approach to pain management. The risk arises specifically from direct, prolonged, repeated skin contact - and that risk can be meaningfully reduced with relatively simple adjustments to how heat is applied. More on this in the prevention section.
Older adults
Older adults remain a recognised risk group, particularly in the UK context. Sitting close to a space heater or open fire for warmth - often for extended periods during colder months - is a long-established cause of the shin presentations historically associated with the condition. Reduced skin sensitivity with age can also mean that discomfort from prolonged heat contact is less apparent, allowing exposure to continue longer than it might in younger individuals.
Children and adolescents
An emerging pattern in clinical literature involves children and teenagers who use laptops resting directly on their thighs for extended periods - particularly during gaming or study. Younger skin is generally more sensitive, and the combination of higher laptop temperatures and long, uninterrupted sessions creates a meaningful exposure risk. Several case reports in the medical literature have described laptop-induced erythema ab igne in adolescents.
Occupational exposure
While less common than it once was, occupational risk remains relevant in certain settings. Those working near industrial heat sources — including professional kitchens, glassblowing, metalwork, and similar environments - may develop the condition through workplace exposure rather than domestic habits.
In practice, the majority of cases seen today involve domestic heat use, often in the context of pain management or prolonged device use. The condition does not follow a single, narrow demographic profile - but understanding where the risk concentrates helps to put individual habits in context.
How Does Toasted Skin Syndrome Develop?
Toasted skin syndrome develops through cumulative heat damage to the skin's surface vessels and cells. Learn what happens beneath the skin and why changes can take months to appear.
Understanding the mechanism behind toasted skin syndrome helps to explain why it can appear without warning after months of apparently uneventful heat use - and why early action, once it is noticed, makes a practical difference to the outcome.
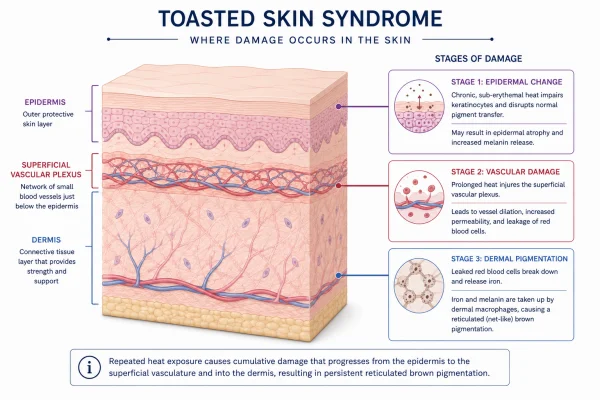
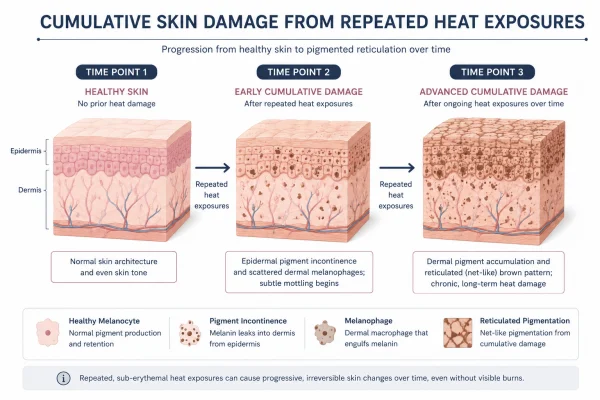
The process begins below the surface
The skin changes associated with toasted skin syndrome do not happen in a single session. They are the result of cumulative stress to the epidermis (the outermost layer of skin) and the superficial vascular plexus - the network of small blood vessels that sits just beneath it.
When skin is exposed to heat in the 43°C to 47°C range repeatedly, several processes begin to occur:
- Vascular dilation: The superficial blood vessels widen in response to heat. Initially, this is a normal, reversible response. With repeated exposure, the vessels lose their ability to return to their resting state and become persistently dilated. This produces the earliest visible sign of the condition - a fixed redness or blotchy discolouration in the affected area.
- Elastic fibre degradation: The connective tissue fibres that give skin its structure and resilience are gradually damaged by sustained heat exposure. Their breakdown contributes to the textural changes and mild atrophy sometimes seen in more advanced cases.
- Melanin release: Heat-induced damage to the basal layer of the epidermis disrupts melanocytes - the cells responsible for pigment production. This triggers an irregular release of melanin into the surrounding tissue, producing the brown discolouration characteristic of the condition.
- Haemosiderin deposition: As blood vessels are repeatedly stressed, small amounts of haemosiderin - a pigment derived from the breakdown of haemoglobin in red blood cells - are deposited in the dermis. This contributes to the deeper, more persistent brown or grey-brown tones seen in established cases.
Why the pattern looks the way it does
The reticulated, net-like appearance of toasted skin syndrome is a direct reflection of the underlying vascular anatomy. The discolouration follows the pattern of the superficial blood vessel network, which is why it presents as an interlocking web rather than a uniform patch. The fishnet or lace-like description used in clinical literature refers to exactly this - pigmentation tracing the skin's vascular structure in the affected area.
The timeline is gradual and variable
One of the more confusing aspects of toasted skin syndrome, from a patient perspective, is that the skin may show no visible change for a considerable period - sometimes weeks, sometimes months - before the first signs appear. The underlying damage is accumulating during this time, but the visible threshold has not yet been reached.
Several factors influence how quickly changes become apparent:
- The temperature and duration of each exposure session
- How frequently the heat source is used
- The sensitivity and thickness of the skin in the affected area
- Individual variation in how skin responds to thermal stress
This variability is clinically relevant. Two people with similar heat use habits may not develop visible changes at the same rate, and the absence of visible symptoms early on does not confirm that no damage is occurring.
What changes if exposure continues
In most cases, removing the heat source once the rash is noticed is sufficient to halt the progression. The skin's natural repair processes can address early-stage changes, though the timeline for visible improvement varies. In cases where exposure continues unchecked - particularly over years rather than months - the structural changes become more entrenched. Pigmentation deepens, the affected skin may thin slightly, and the likelihood of full resolution diminishes. This is the context in which the small but documented risk of long-term complications becomes relevant.
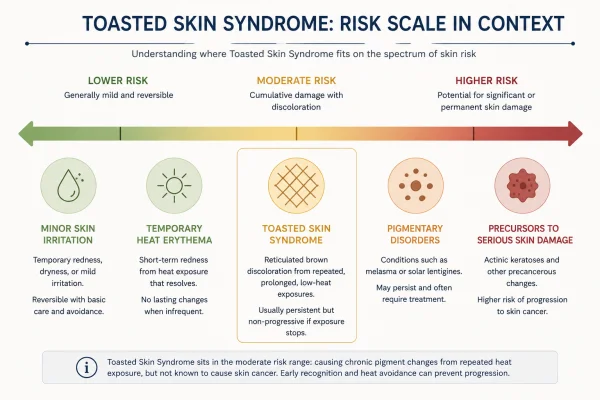
Is Toasted Skin Syndrome Dangerous?
Toasted skin syndrome is usually benign. Learn about permanent pigmentation risk, the rare cancer association, and when to see a doctor.

For most people, toasted skin syndrome is a benign condition that resolves without lasting consequences once the heat source is removed. That reassurance is genuine and evidence-supported. At the same time, there are circumstances where the condition warrants closer attention - and being clear about those circumstances is more useful than either dismissing the risk entirely or overstating it.
In the majority of cases, it is not serious
When toasted skin syndrome is identified reasonably early, and the heat source is removed or significantly reduced, the prognosis is generally good. The rash fades over time, the skin returns to a normal appearance in most cases, and no further intervention is required. The condition itself - at this stage - does not cause systemic harm, is not contagious, and is not a sign of an underlying disease process.
Mild itching or a low-grade burning sensation are occasionally reported, but many people experience no symptoms beyond the visible discolouration. In the early stages, the condition is largely a cosmetic concern rather than a medical one.
Permanent pigmentation is a realistic possibility
That said, toasted skin syndrome does not always resolve completely, and it is worth understanding when permanent change becomes more likely.
If exposure continues for an extended period - particularly where the pigmentation has deepened, and the skin has begun to show signs of atrophy - full resolution becomes less certain. The discolouration may persist indefinitely, even after the heat source has been removed. This is not a dangerous outcome in clinical terms, but it is one that concerns many people and may require active treatment.
The likelihood of permanent pigmentation is broadly proportional to the duration and severity of exposure. Early-stage cases carry a much better outlook than those where heat use has continued, unchecked, for months or years.
The cancer risk: what the evidence actually shows
This is the aspect of toasted skin syndrome that generates the most anxiety - and the most uneven coverage in general health content. The evidence deserves a measured reading.
There are documented cases in the medical literature of malignant transformation arising in areas of long-standing erythema ab igne. The skin cancers most associated with the condition include squamous cell carcinoma (SCC), and rarer cases involving basal cell carcinoma and Merkel cell carcinoma have also been reported. A 2025 update to StatPearls - a continuously reviewed clinical reference - confirms that prolonged exposure carries "the potential for transformation into premalignant or malignant skin lesions."
However, several important qualifications apply:
- The evidence base consists primarily of case reports rather than large-scale population studies. The absolute risk remains low.
- A September 2025 review published in Life (MDPI) explicitly characterises the risk of malignant transformation as rare and "supported only by low-level evidence."
- Malignant change is associated with severe, long-standing, and untreated cases - not with typical short- to medium-term heat use.
- The risk is not considered comparable to, for example, cumulative UV exposure from sun damage, which carries a substantially better-characterised and higher absolute risk.
The practical implication is not that toasted skin syndrome should be treated as a cancer risk for most people who develop it. It is those cases which have been present for a long time, or which show specific warning signs, that merit professional review rather than ongoing self-management.
Warning signs that require medical attention
Certain changes within or around an area of toasted skin syndrome should prompt a GP visit without delay:
- A sore, nodule, or raised area that is not healing
- A change in the texture or surface of the rash - particularly thickening, ulceration, or crusting
- Bleeding or persistent tenderness in the affected area
- Any rapid change in the appearance of established discolouration
These are not signs that cancer is present - they are signs that a clinical assessment is needed to rule it out. In most cases, the examination will be reassuring. The point is that self-monitoring matters, and that changes outside the expected pattern of a stable, fading rash should not be left unreviewed.
Toasted skin syndrome is, in the vast majority of cases, a benign and manageable condition. The cancer association is real but rare, context-dependent, and most relevant to long-standing, severe presentations. Knowing what to watch for is the most useful thing a reader can take from this section.
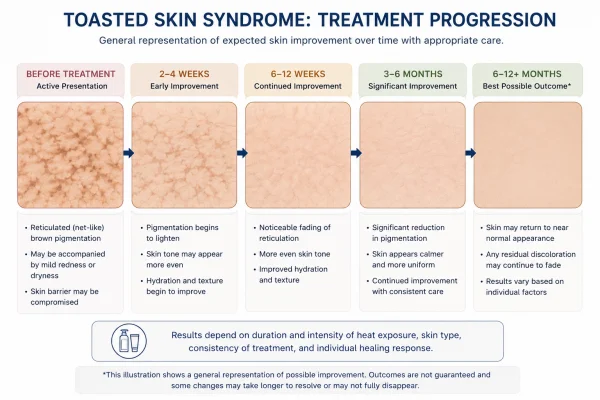
How Is Toasted Skin Syndrome Treated?
Learn about topical options, prescription treatments, and aesthetic procedures for persistent pigmentation.

Treatment for toasted skin syndrome follows a clear, logical progression, starting with the simplest and most effective intervention and moving towards more targeted options as needed. There is no single prescribed treatment pathway - the right approach depends on the condition's severity, how much the discolouration has settled, and the individual's priorities.
Step one: remove the heat source
This is the most important step, and in early-stage cases it is often the only one needed. Removing or significantly reducing contact with the responsible heat source halts further damage accumulation and allows the skin's natural repair processes to begin. For many people, this alone is sufficient - the discolouration fades gradually over weeks to months, and no further treatment is required.
In practice, removal does not always mean abandoning heat entirely. For people using heat to manage pain, the more realistic goal is adjustment: using a barrier between the heat source and the skin, reducing session duration, lowering the temperature setting, or alternating heat with other pain management approaches. The aim is to eliminate or substantially reduce direct, sustained skin contact rather than to remove heat as a tool altogether.
Topical treatments for persistent discolouration
Where the rash does not fully resolve after removing the heat source, or where discolouration has already progressed to a more established stage, topical treatments can support skin recovery and help address residual pigmentation.
Options used in clinical practice include:
- Retinoids (adapalene to tretinoin): Vitamin A derivatives that accelerate skin cell turnover, support the renewal of the epidermis, and can help to fade pigmentation over time. Available in varying strengths, prescription-strength tretinoin is more potent than over-the-counter alternatives.
- Hydroquinone: A topical skin-lightening agent that works by inhibiting melanin production. Used under dermatologist supervision, typically for a defined period, given the potential for skin sensitivity with prolonged use.
- Niacinamide: An anti-inflammatory ingredient that helps to reduce discolouration and supports the skin barrier. Available over the counter and generally well tolerated.
- Vitamin C serums: Antioxidant formulations that can brighten uneven pigmentation and contribute to a more even skin tone. Useful as a supportive measure rather than a primary treatment.
These options are most effective in earlier-stage presentations. In cases where pigmentation has been present for some time and the structural changes to the skin are more established, topical treatments alone may produce limited improvement.
Prescription options for more advanced or at-risk cases
Where the condition has progressed, and there is concern about cellular changes in the skin, a dermatologist may recommend:
- Topical 5-fluorouracil (5-FU): A topical chemotherapy agent used in dermatology to target abnormal or dysplastic skin cells. It is not a first-line treatment for straightforward toasted skin syndrome, but it is used in cases with keratinocyte abnormalities or concern for early premalignant change. It may also reduce the risk of progression in long-standing cases.
- Imiquimod: An immune-modulating topical agent sometimes used in dysplastic presentations, reserved for cases where clinical assessment indicates a need.
These are prescription-only treatments, used under a dermatologist's guidance. They are not appropriate for routine or self-directed management of toasted skin syndrome.
Aesthetic and procedural treatments
For those with persistent cosmetic concerns that have not resolved with topical measures, procedure-based options are available through aesthetic dermatology and medical aesthetics clinics. These are not medical treatments for the condition itself - they address the residual pigmentation once the underlying cause has been managed.
Options that may be considered include:
- Intense Pulsed Light (IPL): A light-based treatment that targets pigmented cells in the skin. Can improve the appearance of reticulated discolouration with a course of sessions, though results vary depending on skin tone and the depth of pigmentation.
- Fractional laser resurfacing: Stimulates collagen production and accelerates skin renewal. May improve both texture and pigmentation in more advanced presentations. Multiple sessions are typically required.
Both options should be approached through a qualified, registered practitioner with experience in treating post-inflammatory and heat-induced pigmentation. A thorough consultation - including a clear history of the condition and confirmation that the heat source has been removed - should precede any aesthetic intervention.
That said, aesthetic treatment is not appropriate for everyone, and realistic expectations matter. In cases where structural skin changes are significant, procedural treatments can improve appearance but are unlikely to fully restore the skin to its pre-exposure state.
When Should You See A Doctor About Toasted Skin Syndrome?
Not all cases of toasted skin syndrome need medical attention. Learn when to monitor at home, when to see your GP, and which signs require prompt review.

For most people, toasted skin syndrome does not require urgent medical attention. Removing the heat source and monitoring the skin are reasonable first responses in mild, early-stage cases. That said, there are circumstances where professional assessment is the right next step - and knowing what those are removes the uncertainty about when to act.
When it is reasonable to monitor at home
If the rash is mild, the pattern is consistent with what has been described in this guide, and you have a clear and recent history of heat exposure in the affected area, it is generally reasonable to begin by removing or reducing the heat source and observing whether the skin improves over the following weeks.
Home monitoring is most appropriate where:
- The discolouration is relatively faint and has not been present for a long time
- The rash is not causing pain, tenderness, or significant itching
- There are no raised areas, nodules, or surface changes beyond discolouration
- The pattern is stable and not changing rapidly
In these circumstances, a watchful approach combined with the preventive measures outlined in the previous section is a sensible starting point.
When to see your GP
A GP appointment is advisable if:
- The rash has not improved after several weeks of removing the heat source
- The discolouration is spreading, deepening, or changing in character
- The affected area is persistently itchy, tender, or uncomfortable
- You are unsure whether what you are seeing is toasted skin syndrome or something else
- The condition is causing significant cosmetic concern, and you would like guidance on management options
- You have been using heat regularly for a long period and want the area reviewed as a precaution
In the UK, a GP can make an initial clinical assessment based on the appearance of the rash and your health history. For straightforward presentations, this is often all that is needed. The GP may recommend a period of watchful waiting, suggest a topical treatment, or refer you onward, depending on what they find.
Red flag signs that require prompt review
Certain changes within or around an area of toasted skin syndrome should prompt a GP visit without delay - not because they indicate a definite problem, but because they warrant examination to rule one out:
- A sore, ulcer, or area of skin that is not healing
- A raised nodule, thickened patch, or new growth within the rash
- Bleeding or crusting in the affected area
- Rapid or unexpected change in the appearance of established discolouration
- Persistent pain or tenderness localised to the rash area
These are not common findings in straightforward toasted skin syndrome. Their presence does not confirm anything serious, but it does mean that self-monitoring is no longer sufficient and that clinical assessment should not be delayed.
When a dermatologist referral is appropriate
Not all cases need to go beyond a GP assessment, but referral to a dermatologist is appropriate in certain circumstances:
- Where the diagnosis is uncertain, a skin biopsy may be needed to confirm it or rule out other conditions
- Where warning signs are present that require specialist assessment
- Where the pigmentation is persistent, established, and the individual is seeking active treatment beyond what a GP would typically prescribe
- Where there is a long history of significant heat exposure, a precautionary review of the skin is warranted
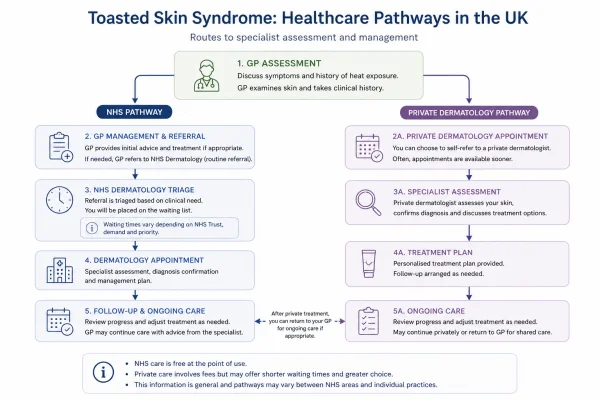
In the UK, NHS dermatology referrals are made through a GP. Waiting times vary by region and by the urgency assigned to the referral. For those with cosmetic concerns or a preference for faster access, private dermatology consultations are available directly without a GP referral, typically with shorter waiting times.
A note on aesthetic clinic consultations
For people whose primary concern is residual pigmentation rather than an undiagnosed or medically significant presentation, a consultation with a qualified medical aesthetics practitioner may be an appropriate route - particularly where IPL or laser treatment is being considered. A reputable clinic will take a thorough history, confirm the diagnosis has been established, and assess suitability before recommending any treatment. Any clinic that proceeds to treatment without this kind of assessment is not following best practice.
It is worth confirming that the heat source has been fully removed before attending any aesthetic consultation. Practitioners typically require this as a prerequisite to treatment, and for good reason: treating residual pigmentation while the underlying cause persists will not produce lasting results.
Toasted Skin Syndrome Quick FAQs
Clear, Concise Answers to Common Queries
A simple, no-fluff roundup of frequent Toasted Skin Syndrome questions to help you get the facts fast.

Is toasted skin syndrome the same as a heat rash?
No, the two conditions are distinct. Heat rash (miliaria) is caused by blocked sweat glands and typically presents as small red bumps or blisters, often with itching or prickling. Toasted skin syndrome results from repeated infrared heat exposure damaging the superficial blood vessels and skin cells over time, producing a fixed, net-like pattern of discolouration. Heat rash tends to resolve quickly once the skin cools; toasted skin syndrome develops gradually and may persist for months after heat exposure stops.
Can toasted skin syndrome develop from a single long exposure?
It is unlikely. The condition is characterised by cumulative damage from repeated exposure rather than a single incident. A one-off session with a heating pad or laptop is not considered a significant risk. The pattern that leads to toasted skin syndrome typically involves the same heat source being applied to the same area of skin regularly over weeks or months. That said, the timeline varies between individuals, and some people may show visible changes sooner than others depending on skin sensitivity and the temperature involved.
Does toasted skin syndrome hurt?
In most cases it does not cause significant discomfort. Some people report mild itching or a low-grade burning sensation in the affected area, but many experience no symptoms beyond the visible discolouration. If the affected area becomes persistently tender, painful, or develops surface changes such as thickening or ulceration, this warrants a GP review rather than continued self-monitoring.
Can children get toasted skin syndrome?
Yes. Children and adolescents are an emerging risk group, primarily through prolonged use of laptops rested directly on their thighs during gaming or study. Younger skin is generally more sensitive to sustained heat exposure, and the combination of higher laptop temperatures and long uninterrupted sessions creates a meaningful cumulative risk. Parents and carers who notice an unusual mottled pattern on a child's thighs or abdomen should consider recent heat exposure habits as a possible cause and seek GP advice if the pattern persists.
Is toasted skin syndrome more common in winter?
It tends to be more prevalent during colder months in the UK, when the use of hot water bottles, electric blankets, space heaters, and fires increases significantly. However, it is not exclusively a winter condition. Heating pad use for chronic pain management, heated car seats, and laptop use occur year-round and can cause the condition regardless of season. The winter pattern is largely a reflection of increased heat source use rather than any seasonal change in the skin's vulnerability.
Can toasted skin syndrome be mistaken for another condition?
Yes, and this is one reason a clinical assessment is sometimes necessary. The reticulated pattern of toasted skin syndrome can resemble livedo reticularis, a vascular condition that produces a similar net-like discolouration but has different causes and implications. It may also be confused with certain types of pigmentation disorders or early skin changes of other causes. A GP or dermatologist can differentiate between these conditions based on clinical appearance and a thorough history of heat exposure. If the diagnosis is uncertain, a skin biopsy may be recommended.
Does toasted skin syndrome affect all skin tones equally?
The underlying condition affects all skin tones, but its visibility varies. On lighter skin, the early erythema (redness) tends to be apparent at a relatively early stage. On darker skin tones, the initial redness may be considerably harder to detect, meaning the condition is often not identified until the pigmentation has progressed to a more noticeable brown or grey-brown discolouration. This can lead to later diagnosis and, in some cases, a more established presentation by the time it is recognised. Anyone who uses heat sources regularly should periodically check the skin in those areas regardless of skin tone.
Can toasted skin syndrome occur on the face?
It is uncommon on the face but not impossible. Facial presentations have been documented in people who regularly hold heat packs or warm compresses against their face for pain relief — for example, to manage jaw pain, sinusitis, or headaches. The face is not a typical site because most heat sources that cause the condition are applied to the torso, limbs, or back. If an unusual reticulated pattern appears on the face in the context of regular localised heat use, it is worth raising with a GP or dermatologist for assessment.
How is toasted skin syndrome different from a burn?
A burn results from heat intense enough to cause immediate tissue damage — typically at temperatures above 48°C to 50°C — and presents acutely with redness, blistering, or tissue destruction. Toasted skin syndrome occurs at lower temperatures, between 43°C and 47°C, where no immediate damage is felt but cumulative exposure gradually disrupts the skin's blood vessels and pigment-producing cells. There is no acute injury with toasted skin syndrome; instead, changes develop slowly over weeks or months of repeated exposure without any single incident causing noticeable harm.
Can men get toasted skin syndrome?
Yes. Although the condition is more commonly reported in women, men can and do develop it. The lower reported prevalence in men is generally attributed to differences in heat use habits rather than any biological difference in skin vulnerability. Men who regularly use heating pads for back or muscle pain, work in warm occupational environments, or use laptops for extended periods on their laps carry the same underlying risk. The condition does not discriminate by sex — it reflects the pattern and duration of heat exposure.
Is there a link between toasted skin syndrome and an underlying health condition?
In some cases, yes. Toasted skin syndrome developing in an unusual location, or in someone without an obvious heat source history, can occasionally prompt investigation into underlying conditions that cause chronic localised pain — since prolonged heat use is sometimes the first visible indicator of unmanaged or undiagnosed pain. Conditions including endometriosis, chronic pelvic pain, and musculoskeletal disorders have all been associated with presentations of erythema ab igne as a secondary finding. A GP may enquire about pain management habits as part of a broader assessment.
Will makeup or fake tan cover toasted skin syndrome?
Cosmetic products can temporarily conceal the discolouration, but they do not affect the underlying condition or its progression. Using makeup or self-tanner over an active or unresolved area of toasted skin syndrome may make early monitoring more difficult, as it can obscure changes in the rash that would otherwise be visible. If concealment is a priority, it is advisable to ensure the heat source has been removed and the skin is being monitored regularly so that any concerning changes are not missed.
Can IPL or laser treatment make toasted skin syndrome worse?
Proceeding with light-based or laser treatments before the underlying heat exposure has been addressed is unlikely to produce lasting benefit and may, in some cases, cause additional skin stress. These treatments are most appropriately used after the heat source has been removed and the skin has had time to stabilise. A qualified practitioner should take a full history before recommending any energy-based treatment for residual pigmentation, and will typically advise against treatment on actively affected or recently exposed skin. Suitability varies depending on skin tone, the depth of pigmentation, and the overall condition of the skin.
How long does it take for toasted skin syndrome to fade after stopping heat exposure?
The timeline varies considerably between individuals and depends on how advanced the condition is. In early-stage cases, gradual improvement may be visible within a few months of removing the heat source. More established pigmentation can take considerably longer — in some cases a year or more — and may not resolve fully without topical or procedural support. There is no fixed recovery timeline, and managing expectations realistically is important. If there is no visible improvement after several months of consistent heat avoidance, a GP or dermatologist review is advisable.
Is toasted skin syndrome covered by the NHS?
Diagnosis and clinical management of toasted skin syndrome is available through the NHS. A GP can assess the condition, confirm the diagnosis, and provide guidance on management. Where a dermatology referral is needed — for example, if the diagnosis is uncertain, a biopsy is required, or the presentation is atypical — this can be arranged through the standard NHS referral pathway, though waiting times vary by region. Cosmetic treatment for residual pigmentation, such as IPL or laser therapy, is not available on the NHS and would need to be accessed through a private aesthetic or dermatology clinic.