

Dry eye affects a significant number of people in the UK, yet many go months or even years before getting a clear explanation of what is happening or how to address it. Part of the problem is the name itself. "Dry eye" suggests a straightforward lack of moisture, when in reality the condition involves a more complex interplay of tear film instability, gland dysfunction, and inflammation. That gap between what people assume and what is actually going on often leads to the wrong products being used, or the right ones being abandoned too early.
Understanding the mechanisms behind dry eye matters because it directly shapes which approaches are most likely to help. A treatment that targets tear evaporation will do little for someone whose issue is primarily reduced tear production, and vice versa. The condition also sits on a broad spectrum, ranging from occasional mild discomfort to a chronic problem that affects work, sleep, and quality of life. Where you sit on that spectrum and what is driving your symptoms determine the most appropriate path forward.
This guide works through the condition step by step: what dry eye is, how it develops, what the symptoms look and feel like, how it is diagnosed and treated in the UK, and what realistic management looks like over time. It draws on current UK clinical guidelines, international consensus reports, and practical considerations that are often missing from online information.
We will start with what dry eye actually is, why the condition is more complex than it sounds, and how the two main types differ.
What Treatment Can And Cannot Do
One of the most important things to understand about dry eye is that it is, in most cases, a chronic condition. That does not mean it cannot be improved, often significantly, but it does mean that the goal of treatment is management rather than cure. Setting realistic expectations from the outset tends to lead to better outcomes and less frustration, because it shifts the focus from searching for a single fix to building a sustainable approach that keeps symptoms under control over time.
Chronic management vs cure
Dry eye disease is usually not curable. NICE CKS states this plainly: symptoms can generally be improved with treatment and modification of underlying causes, but the condition tends to persist, with fluctuating severity and variable duration depending on what is driving it. The glands, surfaces, and processes involved do not typically reset permanently after a course of treatment.
This is not a reason for pessimism. Most people with dry eye can reach a point where their symptoms are well-controlled and their daily life is minimally affected. But it does mean that treatment is ongoing. The warm compresses, the lid hygiene, the lubricating drops, these are not temporary measures you stop once things feel better. They are maintenance strategies, much like managing any other long-term condition.
For some people, particularly those whose dry eye is linked to a specific and modifiable cause such as a medication side effect, a contact lens problem, or an environmental trigger, addressing that cause can produce a near-complete resolution. These cases are the exception rather than the rule, but they do happen, which is one reason why identifying contributing factors matters so much.
Realistic timelines for improvement
One of the more common sources of frustration is expecting rapid results from treatments that work gradually. Different interventions have different timescales, and knowing this in advance can make the process considerably less discouraging.
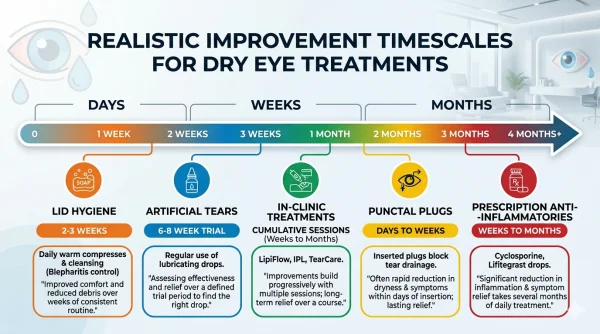
- Lifestyle measures and lid hygiene typically require at least two to three weeks of consistent, twice-daily practice before noticeable improvement begins. The meibomian glands do not unblock overnight, and the ocular surface needs time to stabilise once the tear film starts to improve.
- Artificial tears provide some immediate symptom relief, but finding the right product and formulation often takes several weeks of trial. A reasonable test period for any single product is six to eight weeks before deciding whether it is working.
- Prescription anti-inflammatory treatments such as topical ciclosporin (Ikervis) work by suppressing the chronic inflammatory cycle on the ocular surface. This is not an overnight process. It can take several weeks to months for the full benefit to become apparent, and some people experience initial stinging or discomfort that settles as treatment continues. NICE recommends reassessing the response at least every six months.
- In-clinic treatments such as IPL or Tixel are typically delivered as a course of three or more sessions over several weeks. Improvements in gland function and symptom scores tend to accumulate over the course rather than appearing after a single session. Some people notice a difference within days of the first treatment; for others, the benefit becomes clear only after the course is complete. Maintenance sessions may be recommended annually or as symptoms dictate.
- Punctal plugs can produce a relatively rapid change in tear retention, sometimes noticeable within days. However, the initial trial with temporary plugs is important to ensure the effect is beneficial rather than causing excessive watering.
The overall pattern is that dry eye treatment rewards patience and consistency. Quick fixes are rare. Gradual, sustained improvement is the more typical trajectory, and it is worth building that expectation into your approach from the start.
Why don't all treatments work for everyone
Dry eye is not a single condition with a single mechanism, which is why no single treatment works universally. Someone whose primary problem is meibomian gland dysfunction may see significant improvement from warm compresses and Tixel but little benefit from increasing the volume of aqueous tears. Conversely, someone with aqueous-deficient dry eye linked to Sjogren's syndrome may need intensive lubrication and anti-inflammatory therapy but gain little from gland-focused interventions.
This is compounded by individual variation. Two people with apparently similar clinical findings may respond quite differently to the same product or procedure. The reasons are not always clear and can include differences in nerve sensitivity, inflammatory load, hormonal status, environmental exposure, and adherence to the treatment regimen.
In practice, this means that a degree of trial and adjustment is normal and expected. Trying one eye drop and finding it unhelpful does not mean drops do not work for you. It may mean you need a different formulation, a different viscosity, or a preservative-free option. Similarly, a warm compress routine that feels ineffective after a week may simply need more time, better technique, or adequate heat retention from the compress itself.
The stepped approach used in UK clinical practice is designed to account for this variability. Starting with the simplest measures and building upwards allows treatment to be matched to your individual pattern rather than applying a protocol that assumes everyone responds the same way.
The evidence behind common treatments
It is worth being transparent about the state of the evidence. A comprehensive overview of systematic reviews on dry eye treatments, published in JAMA Ophthalmology in 2024, found that although there was some evidence supporting most recommended interventions, the certainty of that evidence was generally low. Many studies were small, short-term, or inconsistent in their measurement of outcomes. The authors concluded that the conduct and reporting of systematic reviews for dry eye interventions warrant improvement.
This does not mean the treatments do not work. It means that the research has not yet reached the point where definitive statements can be made about exactly how effective each option is, for whom, and for how long. In clinical practice, the treatments recommended by NICE, the College of Optometrists, and the TFOS DEWS II report are based on the best available evidence combined with clinical experience, and most people do benefit from them.
What it does mean for you as a consumer is that healthy scepticism is reasonable, particularly towards marketing claims that promise dramatic or guaranteed results. Any treatment that claims to "cure" dry eye or deliver permanent relief should be approached with caution. The most trustworthy practitioners will be honest about what their treatments can realistically achieve and transparent about the evidence supporting them.
What good management looks like
Effective dry eye management is rarely dramatic. It tends to look like a combination of small, consistent habits: drops used regularly rather than sporadically, a warm compress routine maintained even when symptoms improve, screen breaks taken as a matter of course, and periodic review with a clinician to ensure the approach is still appropriate.
The measure of success is not the absence of all symptoms. For many people, it is a meaningful reduction in discomfort, fewer flare-ups, better tolerance of daily activities, and a sense of control over the condition rather than being at its mercy. That may sound modest, but for someone who has been struggling with persistent grittiness, blurred vision, and the frustration of not understanding what is happening, it represents a significant shift.
The condition may not go away entirely. But with the right approach, it does not have to define your comfort or limit your day.
Your Dry Eye Questions
Real Questions from Real People — Answered
Straightforward answers to the questions people like you are asking right now about Dry Eye.

Be the first to ask a Dry Eye question.
Click here to ask your own question.
Find A Verified Clinic
Trusted Dry Eye Experts, Local to You
Easily connect with qualified, verified professionals for safe, reliable treatment.

To find a Dry Eye clinic near you, please click here.