Our bodies need food as a source of energy for any physical activity that we do, this energy is measured in calories.
As we eat, our digestive system breaks down the food into energy that can be absorbed by our bloodstream and distributed around the body to be used as fuel by our muscles, organs and other tissues.
In order to be healthy, we must all try and balance the amount of calories we consume with the amount of calories that our body burns up. Hence, weight gain, and ultimately obesity, is caused by taking in more calories than we currently use. (There are other medical causes associated with obesity as well).
This is why, as well as eating a balanced diet, it is always advisable to exercise so that we are able to burn up these calories, as when we have taken in more calories than we need the body converts this spare energy source into fat and stores it away, meaning that we gain weight.
In order to establish whether a person is of a healthy weight, or under or over weight, a Body Mass Index (BMI) calculation is used; which basically compares your height with your weight to make sure that your body mass is of a reasonable level.
Why not use the NHS website to calculate your BMI here.
Normally men should have a BMI of between 20 and 25, and women between 18.5 and 23.6. It is also worth noting that although extra fat storage is the commonest reason for a high BMI score, people who are very fit and muscular, such as body builders will also demonstrate a high BMI due to muscle bulk.
A person is categorised as obese if they have a BMI over 30, those with a BMI over 40 are classed as morbidly obese, and those over 50 as super obese. Generally those classed as morbidly obese and above are suitable for bariatric surgery, but cases vary on a person by person basis (see more information below).
According to the National Audit Office (NAO) in 2001, who carried out a report entitled “Tackling Obesity in England”, 1 in 5 adults were obese with the number having trebled over the last 20 years, and nearly two thirds of men and one third of women were overweight or obese.
The NAO stated at the time that;
“The growth of obesity in England reflects a world-wide trend which is most marked in, though not restricted to, developed countries. Most evidence suggests that the main reason for the rising prevalence is a combination of less active lifestyles and changes in eating patterns.”
Obesity is also linked to the onset of various health problems leading to potential death, with the most common problems associated with obesity including heart disease, type II diabetes, high blood pressure and osteoarthritis, thus causing approximately 30,000 deaths a year and an estimated financial impact on the NHS of £5 billion a year in treatment costs for the associated illnesses.
According to the NHS Information Centre, who carried out a 'Health Survey for England 2010' report more recently in December 2011;
"...by 2010, just over a quarter of adults (26% of both men and women) were obese. A further 42% of men and 32% of women were overweight. The rate of increase in the obese population has slowed, however, from an average 0.9% yearly growth between 1993 and 2002 to an average 0.5% yearly growth between 2002 and 2010. Modelling carried out for the Government Office for Science in 2007 suggested that, if trends continued at the current rates, 60% of men, 50% of women and 25% of under-20-year-olds could be obese by 2050."
No major developed nation has so far reversed the upward trend in obesity and the UK as a whole has one of the highest levels of obesity among European countries.
The number of cases of weight-loss surgery performed on obese people by the NHS more than doubled between 2006/7 and 2008/09, the same NHS Information Centre report showed. The NHS performed 4,220 bariatric procedures (which include stomach stapling, gastric bypasses and sleeve gastrectomy) on obese people in 2008/09 compared to 1,950 in 2006/07. The figure also represents a 55% increase on 2007/08 when 2,724 obese people underwent such procedures.
Bariatric surgery is not always available through the NHS; depending on where you live and your particualr circumstances, you may need to seek treatment through a private clinic.
If you are considering bariatric or obesity surgery; the following information will give you a basic understanding of the procedures. It can't answer all your questions, since a lot depends on the individual patient.
Please ask a practitioner about anything you don't understand.
 Surgery In Newnham Bridge")

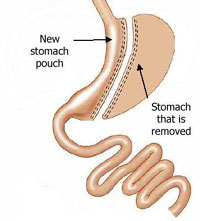
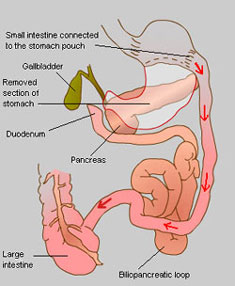 A biliopancreatic diversion (BPD), now superseded by the duodenal switch operation (see below), includes a gastrectomy procedure and the bypassing of most of the small intestines, thus combining restrictive and malabsorptive methods for weight loss.
A biliopancreatic diversion (BPD), now superseded by the duodenal switch operation (see below), includes a gastrectomy procedure and the bypassing of most of the small intestines, thus combining restrictive and malabsorptive methods for weight loss. A duodenal switch operation is based on and includes the biliopancreatic diversion procedure and works primarily by malabsorption, in conjunction with the inherent restrictiveness of removing part of the stomach. This procedure is not widely performed in the UK.
A duodenal switch operation is based on and includes the biliopancreatic diversion procedure and works primarily by malabsorption, in conjunction with the inherent restrictiveness of removing part of the stomach. This procedure is not widely performed in the UK.