
Full Report - Section 2
The rise of regeneration and longevity-led care
If regulation is reshaping structure, regeneration is reshaping clinical philosophy.
Across practitioner, brand and education insights, there is consistent agreement: 2026 will not be defined by more volume or stronger “anti-wrinkle” positioning. It will be defined by tissue health, biological support and long-term planning
The language itself has changed.
“Anti-ageing” is being replaced with:
- Regeneration
- Longevity
- Optimisation
- Skin quality
- Tissue integrity
Patients are not rejecting injectables. They are reframing what they want them to achieve.

What regenerative actually means in practice
Regeneration is often used loosely. The project sources describe something more specific and clinically grounded.
Key areas gaining traction:
- PRP and autologous therapies
- Polynucleotides
- Biostimulators such as CaHA and PLLA
- Exosome-adjacent technologies, with increasing regulatory caution
- Energy-based collagen stimulation
- Combination protocols integrating injectables and devices
Practitioners highlight the move toward collagen stimulation, dermal architecture support and long-term skin function improvement rather than structural overfilling.
Brands reinforce this by focusing on collagen induction, measurable outcomes and biologically driven pathways.
This is not about abandoning traditional toxin and filler. It is about repositioning them within a larger, staged treatment journey.
The cultural driver: Subtlety and authenticity
One of the most important practitioner observations is the decline of over-treatment culture
Patients are:
- More educated
- More aware of unnatural outcomes
- More cautious about permanence
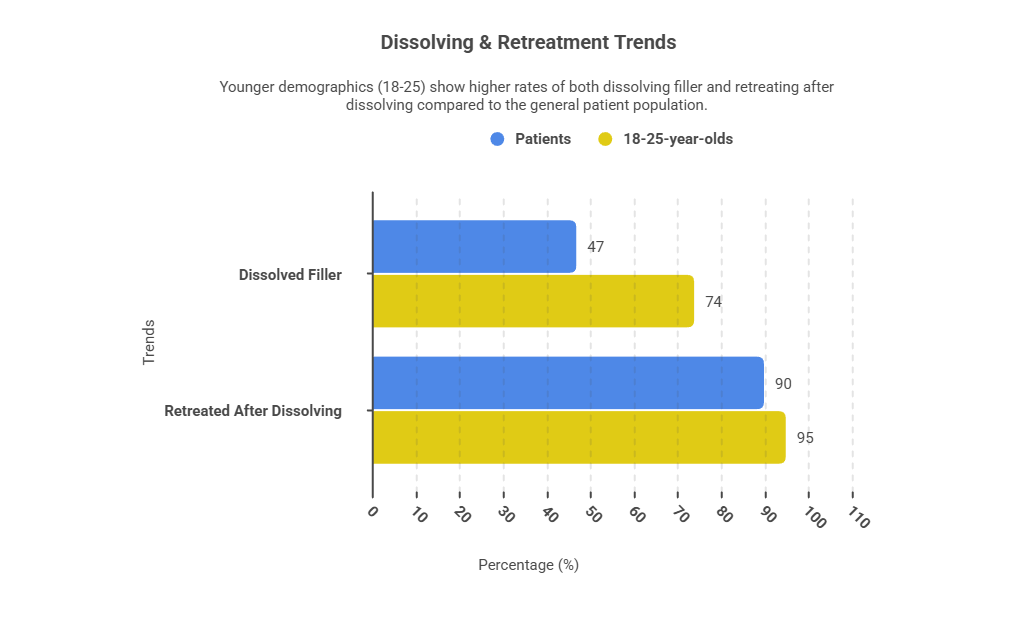
- Increasingly requesting dissolving and retreatment flexibility
The industry conversation around filler dissolving, for example, is becoming more constructive and patient-centred, reinforcing trust rather than signalling failure
Subtlety is no longer a compromise. It is the goal.
Clinics that can articulate regeneration in terms of “supporting what the body already does well” are aligning with patient psychology.
The longevity influence
Longevity medicine is weaving into aesthetic practice more visibly.
- Practitioners anticipate stronger integration of:
- Hormonal health
- Sleep optimisation
- Metabolic awareness
- Menopause-informed planning
- Preventative intervention in younger cohorts
- Practitioners Outlook 2026
Associations and menopause-focused organisations highlight midlife women as a growing demographic requiring nuanced, medically informed approaches
This is not about turning aesthetic clinics into functional medicine centres. It is about acknowledging that skin health is influenced by systemic biology.
Clinics that can responsibly discuss inflammation, collagen biology and hormonal transition without overreaching into unsupported claims will stand out.
Regeneration meets governance
There is also a cautionary thread.
While regenerative treatments are expanding, experienced voices are emphasising evidence, training and regulatory clarity
Some technologies, particularly in the exosome space, are expected to face tighter scrutiny due to legality and safety ambiguity.
The lesson is straightforward:
Innovation without governance will not survive 2026.
Regeneration must be delivered with:
- Documented protocols
- Clear sourcing transparency
- Realistic outcome setting
- Proper complication management
This is where clinics either mature or overextend.
The commercial opportunity
Regeneration is not only clinically aligned. It is commercially intelligent.
Why?
Because regenerative pathways lend themselves to:
- Staged 6–12 month plans
- Membership models
- Layered combination protocols
- Higher retention rates
- Reduced discount dependency
Brands and business advisers repeatedly emphasise programme-based care as a resilience strategy.
A patient on a structured collagen-support pathway is more predictable than a patient chasing one-off aesthetic corrections.
This stabilises revenue and deepens trust simultaneously.
How to operationalise regeneration in 2026
If you want to move beyond trend adoption and into structured implementation, consider this phased approach:
Step 1: Reframe consultation language
Shift from:
“What would you like to fix?”
To:
“How do we want your skin to behave over the next 12 months?”
Step 2: Build layered protocols
Integrate:
- Conservative toxin
- Targeted filler
- Biostimulator or polynucleotide
- Energy-based collagen stimulation
- Medical-grade skincare
- Maintenance review checkpoints
Step 3: Define measurable milestones
Use:
- Photography
- Skin analysis
- Texture scoring
- Patient-reported outcome measures
Regeneration performs best when progress is visible and structured.
The risk of misinterpretation
There is a danger in chasing regenerative language without discipline.
Common pitfalls to avoid:
- Overpromising “stem cell” style results
- Adopting poorly evidenced adjuncts
- Running multiple new modalities without integration
- Positioning regeneration as trend rather than long-term strategy
Experienced clinicians are clear: regeneration must be grounded in tissue biology and anatomy-led planning.
Precision beats novelty.
The bigger picture
Regeneration is not replacing aesthetics.
It is redefining it.
The UK market is moving from:
High-volume correction to Structured biological optimisation.
From Surface change to Tissue behaviour.
From Transaction to Journey.
Clinics that embrace this shift thoughtfully will experience:
- Higher-value patient relationships
- Greater retention
- Stronger differentiation
- Alignment with regulatory direction
Those who continue volume-led, promotion-driven filler models may find themselves increasingly misaligned with patient sentiment.